
Alberta Thoracic Oncology Program (ATOP)
- ALL.CAN CANADA

- Jul 31, 2025
- 8 min read
Updated: Oct 30, 2025

THEMES:
• Timely diagnosis
• Expedited referrals
• Diagnostic assessment
• Multidisciplinary team
• Automation
• Coordinated Care
SUMMARY
Lung cancer has the highest incidence in Canada and remains the leading cause of cancer death, responsible for about 1 in 4 cancer deaths among Canadians.1
Despite this large impact, over the last decade there has been a substantial drop in both the lung cancer incidence and death rates for men and women.
In Alberta, the incidence of lung cancer in both females and males has decreased steadily over time but remained the leading cause of mortality in 2023 mainly because of late stage diagnosis.2
In Alberta, about half of the patients with lung cancer are diagnosed at stage IV (advanced stage) with a five-year survival rate of 13%. Effective lung cancer staging requires a well-coordinated, multidisciplinary approach, yet gaps in communication often lead to redundant testing, misinterpretation of imaging results, and treatment delays. These inefficiencies highlight the urgent need for integrated referral systems that facilitate real-time information sharing and standardized diagnostic pathways.

Early detection and timely intervention are critical for improving survival rates. However, systemic inefficiencies continue to hinder access to prompt diagnosis and treatment, leading to prolonged disease progression and reduced survival outcomes for patients. One of the most significant barriers is the delay in specialist referrals, particularly for patients in rural and remote areas where there is a shortage of oncologists and diagnostic facilities.
Across Canada, including in Alberta, individuals living in rural areas experience notable disparities in access to timely lung cancer diagnosis and treatment when compared to those in urban settings.3

This disparity often results in late-stage diagnoses, limiting treatment options and reducing effectiveness.4 Implementing centralized electronic health records (EHRs) and telemedicine platforms could enhance real-time collaboration among healthcare providers and improve continuity of care.5
Limited access to specialized diagnostic procedures further contributes to disparities in lung cancer outcomes, underscoring the need to expand regional availability of tools like PET scans, EBUS, and mobile diagnostic units. These essential services remain unavailable in certain regions6, forcing patients in southern Alberta, southeast British Columbia, and Saskatchewan to travel long distances—often to Calgary or Edmonton—for care. This travel can present significant logistical and financial barriers, leading to delays in diagnosis and treatment. Research shows that greater travel distances to cancer centers are associated with worse survival outcomes for lung cancer patients.7
A 2016 study8 found that many Albertans with potentially curable non-small cell lung cancer (NSCLC) experienced delays exceeding recommended care timelines. Alberta fell short of both local and international benchmarks for NSCLC diagnosis and treatment:
The median diagnostic interval was 38 days, with the 90th percentile reaching 148 days, indicating significant delays.
Surgical patients faced a median wait time of 105 days from diagnosis to treatment, highlighting a critical gap in timely intervention.
45% of NSCLC patients underwent an initial biopsy attempt that failed to provide a definitive diagnosis, leading to further delays in treatment planning.
These findings underscore the urgent need for systematic improvements to reduce diagnostic and treatment delays and enhance lung cancer care in Alberta. Implementing standardized referral pathways, fostering stronger interdisciplinary collaboration and streamlining access to specialized oncology care7 will be critical in addressing these challenges.
Integrating multiple testing procedures within a seamless multidisciplinary framework presents operational challenges. Coordinating thoracic surgeons, interventional pulmonologists, radiation oncologists, and medical oncologists requires efficient case management to prevent bottlenecks in patient flow.8 Addressing these challenges through a more cohesive and structured approach is essential to improving lung cancer outcomes in the province.
SOLUTION
Established in 2011, the Alberta Thoracic Oncology Program (ATOP) is committed to providing coordinated, efficient, and timely care for patients. ATOP’s expert teams include thoracic surgeons, interventional pulmonologists, and nurse practitioners specializing in thoracic oncology. The program's primary goal is to transform cancer care in Alberta by improving the patient experience, enhancing diagnosis and treatment outcomes, and ensuring a consistent standard of care across the province.
ATOP's multidisciplinary approach facilitates a seamless transition from diagnosis to treatment, reducing delays in lung cancer care pathways.7,9 A prospective, observational, non-randomized study conducted between 2013 and 2015 examined whether allowing radiologists to directly initiate specialist referrals at the time of CT scan interpretation would reduce delays compared to the traditional process, which required referral through another healthcare provider.
Researchers conducted a prospective observational study involving two patient groups referred to the Alberta Thoracic Oncology Program-South (ATOP-S):
Group 1: Patients referred immediately by a radiologist upon detecting a suspicious lesion.
Group 2: Patients referred through a separate healthcare provider (e.g., family physician or general practitioner).
Key time intervals were measured and results (Table 1 & 2) indicated that radiologist-initiated referrals (Group 1) significantly reduced delays in all measured timeframes.

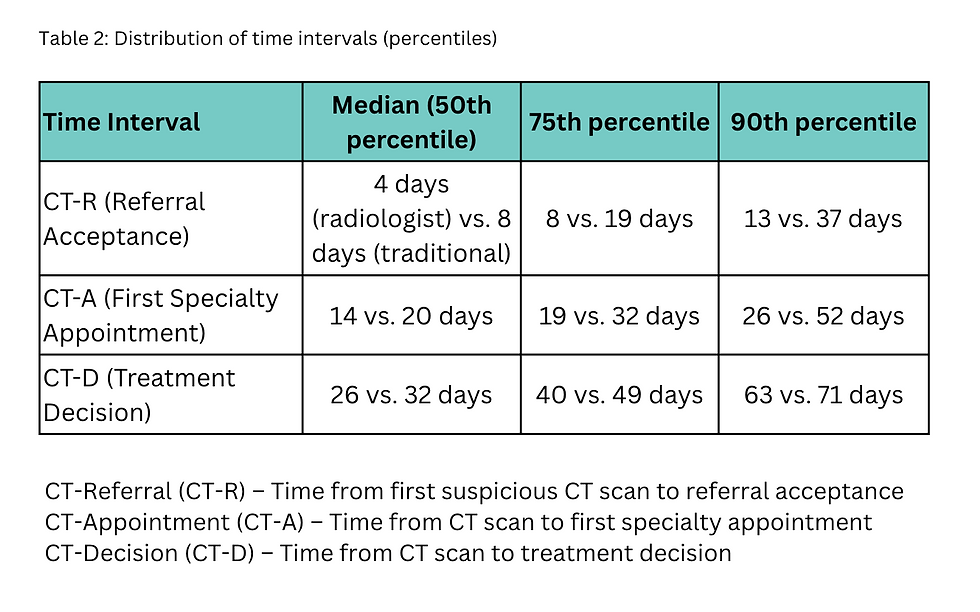
Overall, the study found that a referral from a radiologist contributed to a faster diagnosis, a more efficient workflow and an improved outcome. Patients referred by a radiologist received specialist appointments and treatment decisions 6 days sooner on average than traditional referrals. Allowing radiologists to initiate referrals reduces bottlenecks in lung cancer diagnosis and staging. Earlier specialty consultation may lead to earlier intervention and better treatment outcomes.

Radiologist-initiated referrals accelerate patient access to care.
Time savings range from 4 to 6 days in median cases and up to weeks in worst-case scenarios.
Implementing direct referrals from radiologists could significantly improve lung cancer diagnostic pathways.
ATOP’S AUTOMATIC REFERRAL PROCESS
Human intervention remains a limiting factor, as radiologists must recognize and act on suspicious findings in real-time, potentially introducing variability in response times and workload-dependent bottlenecks.
A 2020 study9 explored the potential of automation in referrals, implementing a system where software detects potential malignancies on CT scans and automatically triggers a referral. This approach removes human dependency, theoretically reducing delays even further than the radiologist-initiated method. To accelerate access to specialist care, ATOP has implemented an automated radiology referral system, which has significantly reduced referral times from 23.6 days to 4.7 days, enabling specialists to review cases in a fraction of the usual time.9 The study aimed to determine whether automatic referrals reduced the time from CT scan to specialist referral and whether they affected the quality of referral information.
A retrospective review of 689 patients was conducted at a Canadian thoracic surgical center to demonstrate the efficiency of automatic referrals (Figure 4). Of these, 405 patients were referred through the automatic system, while the remaining 284 followed the traditional referral process. Patients in the automatic referral system were seen much faster (4.7 days vs. 23.6 days in traditional referrals, p < .001).9

Only 2 automatic referrals took longer than 30 days, compared to over 25% of traditional referrals.
The time savings were consistent across different lung nodule types, physician specialties, and patient locations.
There was no difference in the quality or completeness of referral information between the two groups.

This streamlined process fosters closer collaboration between primary care physicians, radiologists, and thoracic oncology specialists, ensuring that patients receive timely, coordinated, and efficient care.5
The automatic referral system significantly reduced delays in lung cancer diagnosis and treatment, potentially leading to better survival rates and fewer cases of disease progression. These improvements were achieved without compromising the quality of referral data, making automatic referrals a more efficient and effective approach to lung cancer care.
Furthermore, ATOP takes pride in its team of dedicated nurse practitioners, who meticulously review all patient referrals, initiate information intake, and conduct preliminary evaluations, ensuring a comprehensive understanding of each patient's condition.
ACHIEVEMENTS
The Alberta Thoracic Oncology Program (ATOP) has significantly enhanced lung cancer care by implementing swift diagnostic pathways, expedited referrals, and seamless patient care coordination.
One of the key achievements of the Alberta Thoracic Oncology Program-North (ATOP-N) was the successful implementation of a Diagnostic Imaging (DI) Notification process, which significantly improved the timeliness of care for patients suspected of having lung cancer. The DI Notification process has proven to be a novel and effective strategy in optimizing the management of suspected lung cancer cases, ensuring faster access to specialized care and improved treatment decision timelines.5
Through an integrated diagnostic framework, ATOP facilitates rapid identification and staging of lung cancer, utilizing multimodal imaging techniques such as CT scans, PET scans, and EBUS to enhance early detection and diagnostic accuracy.4,6
Endobronchial ultrasound (EBUS) has become a minimally invasive yet highly sensitive tool for lung cancer staging, often replacing mediastinoscopy as the preferred method for lymph node assessment.6,10
While mediastinoscopy remains the gold standard, EBUS-transbronchial needle aspiration (TBNA) has largely replaced it in many clinical settings due to its improved safety profile and comparable diagnostic accuracy.
Minimally invasive techniques such as endobronchial ultrasound transbronchial needle aspiration (EBUS-TBNA) and endoscopic ultrasound-fine needle aspiration (EUS-FNA) have demonstrated high diagnostic yield and low complication rate and have made a significant difference in the time to diagnosis and lives of patients. There continues to be innovation in the field of bronchoscopy with the development of new technologies such as confocal laser endomicroscopy, optical coherence tomography, and artificial intelligence.11
In addition to EBUS, CT-guided transthoracic needle aspiration has demonstrated high diagnostic accuracy for peripheral lung lesions, though it carries a small risk of complications, such as pneumothorax.4
NEXT STEPS
The Alberta Referral Program in collaboration with rapid-access clinics in Edmonton and Calgary serves as a critical hub for evaluating suspected lung cancer cases, ensuring that patients receive prompt assessments and personalized treatment strategies.8 This system enhances collaboration between primary care physicians, radiologists, and thoracic oncology specialists, ensuring patients receive timely and coordinated management.5
ATOP will continue the collaboration with Alberta Health Services, the Cancer Program Improvement and Integration Network (PIN), and Cancer Control Alberta whose support allows ATOP to maintain a superior level of care and service for patients, contributing significantly to ATOP’s mission of providing the best possible patient outcomes.
To effectively address these barriers requires a comprehensive approach, including:
Strengthening referral pathways through automated systems that minimize wait times.9
Expanding access to PET scans and EBUS in underserved regions through mobile diagnostic units or telemedicine-assisted referrals.12
Enhancing coordination between specialists and primary care providers through real-time data-sharing platforms to reduce diagnostic delays.5
Improving financial and logistical support for patients travelling long distances to referral centers to ensure equitable access to care.8
By prioritizing multidisciplinary collaboration, enhancing diagnostic accessibility, and streamlining referral systems, the burden of lung cancer mortality can be significantly reduced, ultimately improving patient survival and quality of care across Canada.
FURTHER INFORMATION
Alain Tremblay
University of Calgary
Calgary, AB
Narender Singh
Alberta Health Services
Calgary, AB
References:
Canadian Cancer Society. (2023). Lung Cancer Statistics Report. Statistics Canada.
Cancer Care Alberta. (2024). 2024 Report on Cancer Statistics in Alberta. Alberta Health Services. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023-province-specific/ab-specific-stats-2023.pdf
Canadian Partnership Against Cancer. (2020). Lung cancer and equity: A focus on income and geography. Canadian Partnership Against Cancer. https://s22457.pcdn.co/wp-content/uploads/2020/11/Lung-cancer-and-equity-report-EN.pdf
Dziedzic, R., Marjański, T., & Rzyman, W. (2021). A narrative review of invasive diagnostics and treatment of early lung cancer. Translational Lung Cancer Research, 10(1), 45–60.
Gillson, A. M., Veenstra, J., Stewart, K., Ruston, T., & Abele, J. (2017). Timeliness of referrals using a diagnostic imaging notification process for patients suspected of having lung cancer. Chest, 152(5), 1041–1050.
Avasarala, S. K., Aravena, C., & Almeida, F. A. (2020). Convex probe endobronchial ultrasound: historical, contemporary, and cutting-edge applications. Journal of thoracic disease, 12(3), 1085–1099.
Tremblay, A., Strilchuk, N., Taghizadeh, N., Fortin, M., Burrowes, P., Hampton, L., … McFadden, S. (2017). Radiologist initiated specialty referral for patients suspected of having a thoracic malignancy. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine, 1(4), 180–185.
Kim, J. O. A., Davis, F., Butts, C., & Winget, M. (2016). Waiting time intervals for non-small cell lung cancer diagnosis and treatment in Alberta: Quantification of intervals and identification of risk factors associated with delays. Clinical Oncology, 28(7), 409–417.
Veenstra, J. S., Khalid, T., Stewart, K. C., Valji, A., Bédard, E. L. R., Johnson, S., Laing, B., & Turner, S. R. (2020). Automatic referral for potential thoracic malignant diseases detected on computed tomographic scan. The Annals of Thoracic Surgery, 110(6), 1869–1873. https://doi.org/10.1016/j.athoracsur.2020.05.040
Czarnecka-Kujawa, K., & Yasufuku, K. (2017). The role of endobronchial ultrasound versus mediastinoscopy for non-small cell lung cancer. Journal of Thoracic Disease, 9(Suppl 10), S967–S978.
Dollin, Y., Pineda, J. A. M., Sung, L., Hasteh, F., et al. (2024). Diagnostic modalities in the mediastinum and the role of bronchoscopy in mediastinal assessment: A narrative review. Journal of Thoracic Oncology.
Ramsahai, J. M., Molnar, C., Lou, L., & Ying, W. (2020). Does prior mediastinal lymph node aspiration contribute to false-positive PET-CT results? ERJ Open Research, 6(4), 00103-2020.


